Answer: I don't know where to begin. Don't smoke. Please read the following.
Smoking is one of the worst things you can do to yourself. If you want to do one thing to improve your health, the best thing you can do is stop smoking.
In regards to your specific question:
- Although not universal, many have people have reported weight gain with smoking cessation. Reasons for this relate to various potential factors.
- Smoking ruins a lot of your taste buds and ability to smell. Therefore the joy of eating is diminished. Less food = less weight.
- If you have a cigarette in your mouth you don’t have food in your mouth, so less food.
- When trying to quit, people replace smoking with snaking.
- Nicotine is an appetite suppressant and stimulant.
- If you get cancer or emphysema from smoking you will definitely lose weight, but probably not the kind of weight loss you are looking for.
- The health benefits of being tobacco free far exceed the problems associated with even moderate weight gain. Smoking is not a viable option for weight control.
- Overall weight control is a simple equation of, "in's and out's." If you can control what goes in (food) and counteract that with what goes out (exercise), you are golden.
Please ask yourself why you want to resort to smoking to lose weight/keep from gaining weight:
- In my experience it can generally be broken into two major reasons why people what to lose weight.
- Some want to lose weight for health reasons.
- Others want to lose weight for looks.
- Regardless of your motivation to lose weight, smoking is not a viable strategy.
- Let me elucidate the reasons.
Lose weight for appearance:
- If you are concerned about appearance, smoking is not the way to go. Smoking will decrease your beauty on every level.
Skin:
- Smoking will accelerate skin ageing. The toxic chemicals in the smoke go throughout your body and damage just about everything it comes in contact with, (this includes your skin).
- The blood vessels that feed your skin (and other organs) are also damaged. No wonder why smokers have prematurely old looking skin.
- Speaking of skin: Smoking is linked to a 2 X increased risk of developing psoriasis.
Teeth:
- The yellow/brown stain on your teeth is only part of it.
- Smoking also damages your salivary glands. A major cause of tooth decay is low saliva (xerostomia). One of the many bad things smoking does is that it causes tooth decay by causing xerostomia.
- Smoking also significantly increases risk for many other dental problems: including oral cancer and gum disease.
- It will take longer for your dentist to clean your teeth. Who wants to spend any more time at the dentists than they need to?
- Smokers do not heal as well after surgeries (tooth extractions, and periodontal procedures included).
Breath:
- You may think that others can’t tell you smoke because you cover it up with mints/deodorant/perfume, etc. Or you think no one will notice because you only smoke at home at night on the back porch. But guess what? You can’t smell as well as others because you smoke. We can smell that nasty. Even if you are lucky and it is very subtle, we can still tell something is off.
Fingers:
- Got that yellow on your fingernails yet? I guess you can put nail polish on. It is hard to cover up the skin stains though.
- Skin just looks old everywhere.
- In addition, some people will have a change in the shape of their fingers because of smoking. The finger tips get a bulbous look from smoking (digital clubbing).
Bones:
- Smokers have weaker bones than nonsmokers. Who wants to be shorter and bent looking?
Hair:
- Smoker's are three to six times more likely to go prematurely gray than nonsmokers.
- A smoker's hair is more brittle, older looking.
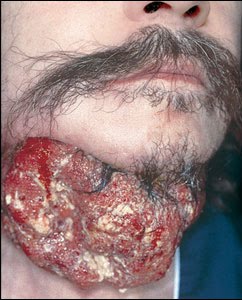
Cancer:
- I have seen a lot of head and neck cancer and surgery for tobacco related tumors. I have seen a lot of bad things in my career and the nasty head and neck cancer always gets me. Even a small cancer (if you’re hoping for the best) will result in a major scar. You ever worry about a pimple? That is nothing. Head and neck surgery is majorly disfiguring (it is the, 'you don't ever want to ever go out of the house kind-of bad').
General:
- Smokers are four times as likely to report feeling unrested after a night's sleep. In regards to appearance, most people look/feel like crap after a bad night’s sleep.
So then you ask yourself, “Why do I want to lose weight-look good.”
- For most it is because they want to have a relationship. Or to be in a position to have/stay in a relationship.
- A 2005 survey of Canadians found that more than half of people surveyed would not date a smoker.
- No one wants to kiss a prematurely ageing, cancer prone, smelly ashtray.
- But if you do get into a relationship beware. Smoking affects circulation; with less blood flow to your genitals, arousal for both men and women can be more difficult. And yes impotence. Bummer.
- Cigarette smoking is a risk factor for developing diabetes. Diabetes causes impotence. Double bummer.
You want to lose weight for health:
- It is almost a joke to explain why smoking is not a healthy way to attempt to lose weight.
- You know tobacco causes lung cancer, emphysema and heart disease. But there is so much more…
Some more tobacco related health badness you might not know:
- Not just lung and mouth cancer. Also significant increased risk of cancer of the throat, Esophagus, Pancreas, Kidney, Bladder, Cervix, etc.
- Smoking also significantly increases the risk for stroke, hypertension, and spontaneous head bleed.
- Tobacco smoke contains four thousand-plus chemicals… most of them bad (cyanide, lead, ammonia, carbon monoxide, etc).
- What did you say? Smokers have a nearly 70% greater likelihood of developing hearing loss than nonsmokers.
- A study in the Netherlands showed that smokers took an average of 11 more sick days a year than nonsmokers.
- Peninsula Medical School surveyed 10,000 and found that smokers reported below average pleasure and satisfaction with their lives than the nonsmokers.
- Smoking increases the risk of depression.
- Smoking = earlier menopause by several years.
- People are allergic to cigarette smoke. Smoking worsens allergies.
- The Canadian Journal of Public Health reported that smokers got into car accidents 1.5x more often than nonsmokers.
- Cigarette smoke doubles your risk of macular degeneration, which is a leading cause of blindness.
- The journal Neurology studied 7,000 people and found that smoking also increases the risk of dementia. What is going on?
- Women who smoke take longer to become pregnant and are more likely to miscarry.
- And by the way: if you're on the Pill and smoke beware. Mixing the two is an extra major risk for acute blood clots, pulmonary embolism, heart attacks, and strokes.
- If you were to take a medical school test and the question was: “what is the one best thing you can do to improve your health” the answer will always be Quit smoking. It doesn’t matter what the other options are.
- Smoking is estimated to be the single largest cause of preventable deaths in the United States.
The health benefits of being tobacco-free far exceed the problems associated with even moderate weight gain. Lung damage and heart disease are irreversible — weight gain is not.
American Cancer Society
Quit smoking: Every cell in your body will benefit.